Uses and Pitfall
- In addition to pre-op localization of insulinoma, GLP-1 receptor imaging also might be used for dynamic evaluation of response to non surgical treatment of insulinoma.
-
It is used in MEN 1 patients, guide surgerical procedures. In MEN 1 patients, aggressive resection of pancreatic neuro-endocrine tumors was previosuly proposed, but it was associated with significant mortality. Recent studies suggests non fucntioning pancreatic neuro-endocrine tumors rarely develop metastases. There is no difference in survival with watchful waiting.
-
Malignant insulinomas are <10% of insulinomas. They lack GLP-1 receptors. They express SSTR-2 receptors.
-
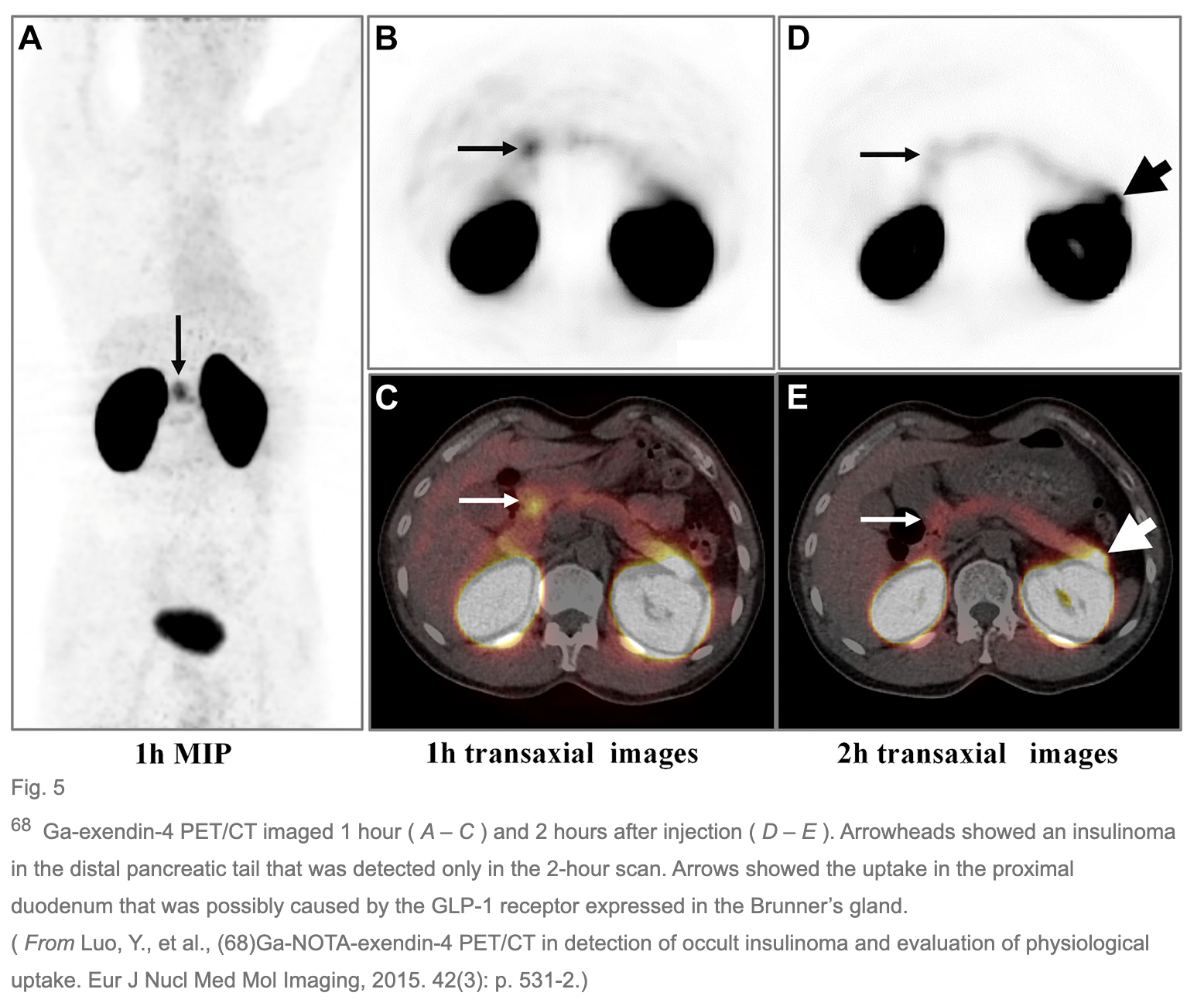
High physiologic expression of GLP-1 receptor is noted in the brunners gland in proximal duodenum, therefore there is physiological uptake in the duodenum, which can lead to false interpretation.
-
Renal excretion of exendin -4 interfere with detection of insulinoma in distal pancreas tail located near to the left kidney. Megalin mediated reabsorption in the proximal tubules after glomerular filtration is responsible for renal retension of tracer.
-
To reduce the reabsorption, infusion with succinylated gelatin- a plasma expander to induce low molecular weight pseudoproteinuria before tracer injection has been suggested. It reduces renal uptake helpinh in better pancreatic tail visualization.
-
18F-TTCOCys40- exendin 4 shows reduced kidney uptake and faster clearance rate.
-
Radiolabelled exendin - 4 derivates with addition of an albumin binding moiety, using antagonistic tracers, using chelator desferrioxamine or through brush border membrane enzyme - mediated degradation with clearance linkers, reduce kidney uptake.
-
Exendin - 4 analogue of GLP-1 causes hypoglycemia. Thus it was suggested that all patients receive an exogenous glucose infusion during PET/CT examination. Nausea and vomiting are other side effects.
-
It can also be used for distinction between insulinoma and nesidioblastosis. Nesidioblastosis is a neogenesis of islet of langerhan cells from pancreatic duct epithelium with primary islet cell hypertrophy.
-
In congenital hyperinsulinism, 18F DOPA is well established to distunguish between focal and diffuse type of nesidioblastosis and thus to guide surgery.
-
L DOPA is a precursor of catecholamines that is converted to dopamine by aromatic AA decarboxylase and pancreatic islets take up L DOPA and convert it to dopamine by AADC. In contrast to infancy, 18F DOPA has limited value in adults, because intense uptake in pancreas in adults due to presence of AADC in exocrine pancreas.
-
Islet transplantation is one of the treatment option for Diabetes patients. Transplanted functional islets can be imaged with a GLP-1 receptor target agent and this approach may have potential for non invasive monitoring of islet cell graft survival after transplantation.
-
GLP-1 receptor imaginng to assess pancreatic Beta cell mass which is a key issue in diabetes mellitus. Considering imaging of beta cell mass is challenging due to low concentration of beta cells in pancreas, which accounts for only 1 to 2 % of total pancreatic mass, the high retention of exendin - 4 in kidneys is complicating beta cell mass quantification by SPECT or PET imaging.
-
The spill in and spill out signal from the highly radioactive kidneys may significantly bias the quantification of the radioactivity levels in the adjacent makedly less radioactive pancreas.
Follow me on Twitter @KoteRutuja for more updates and resources.